Distal Femur Fracture Postoperative Protocol
The Reno Orthopedic Center Fracture and Trauma Surgeons have created postoperative fracture protocols for our patients. These are based on the latest orthopedic science and literature in order to give patients the most up to date care. Their content is designed to explain what type of injury was sustained, the type of surgery that was done and simple instructions for weight bearing, wound care, physical therapy, medicine and diet issues. Patients will hear similar information in each postoperative visit but it is easy to forget what is said. The following protocol is designed to help patients in their healing with a single resource for frequently asked questions.
What Was Broken
You broke the upper bone of your knee which is called the distal femur. Sometimes this crack can go into the knee joint and disrupt the cartilage. It is also common in bone above knee replacements.
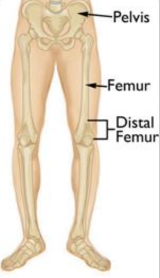
Illustration of distal femur bone. Reproduced with permission from OrthoInfo. © American Academy of Orthopaedic Surgeons. https://orthoinfo.org/

Preoperative CT scan of distal femur fracture.

Preoperative x-ray of distal femur fracture.
What Was Done in Surgery
The broken bone was rebuilt back to its preinjury position and held with a large titanium plate and 7-12 screws. This plate is very thick to make it strong.

Postoperative x-ray of distal femur fracture repair.
Follow Up Appointment
You should see your surgeon or his physician assistant 10-14 days after surgery. Usually, this appointment is made when you schedule surgery. If you do not have one, please call the office to schedule at 775-786-3040 as soon as you can. You will be seen at 2 weeks, 6 weeks and 3 months from surgery where the provider will examine you and x-rays will be taken to follow bone healing.
Brace
You have been given a knee immobilizer after surgery. This keeps your knee out straight to allow the incision to heal without splitting open and protects the bone. You can take the brace off to shower. At your first postoperative visit you will be transitioned to a hinged knee brace that lets your knee bend that you will wear for 4 weeks.
Wound Care
Your wound was closed with either sutures or staples. After 2 days you can take off the dressing. If the wound is dry, you do not need to cover it with a new bandage. If it is leaking, replace dressing with a clean gauze pad and tape.
Showering
You may shower immediately after surgery. Your dressing from surgery is waterproof. If it gets wet, remove the bandage, and place a new one. Do not immerse your wound in a bath or hot tub until your stiches or staples are removed.
Pain Control
You have been given a prescription for narcotic pain medication. You can take 1-2 pills every 4-6 hours. It is ok to take anti-inflammatory medicine like Motrin (ibuprofen) or Tylenol (acetaminophen) as well. Do not take more than 4 grams of Tylenol a day or it can hurt your internal organs. The orthopedic surgeon by law can only give you narcotic pain medicine for 2 weeks after surgery. This must be prescribed in only a 5 day supply each time. If you already get narcotics from your primary care doctor or pain management doctor, the orthopedic surgeon cannot write you a separate prescription. If you need prolonged narcotics, we can refer you to a pain management specialist. If these rules are bent, the orthopedic surgeon can lose his medical license, insurance contracts and be unable to care for other patients like you. Please respect these regulations.
Marijuana
THC and CBD products can be helpful for postoperative pain and decrease the amount of narcotics you need. In Nevada, marijuana is legal, and you do not need a doctor’s prescription to get it. THC use avoids the constipation and addiction potential associated with narcotic use. Edible use avoids the other risks associated with smoke inhalation and has more controllable dosing.
Diet
Eat a well-balanced diet. If you are diabetic keep your blood sugars well controlled. High blood sugar can put you at risk for infection, wound complications and the bone not healing(nonunion).
Smoking
It is recommended that you do not smoke or chew tobacco while your bone is trying to heal. The healing factors for your bone travel in your bloodstream and nicotine constricts blood vessels making your bone heal slower. Smoking increases the risk that your bone will not heal.
Sutures/Staples
Your wound has been closed with sutures or staples depending on your surgeon’s preference. They will be removed at your first postoperative follow up appointment 10-14 days after surgery.
Weight Bearing
There are several types of distal femur fractures. Your surgeon will tell you after surgery if you can put all your weight on your leg or not. If your fracture is in many small pieces or is into the joint, often you will not be able to walk on it right away. You will be toe touch weightbearing immediately after surgery. This means that your foot can rest on the ground but you should not put weight on it. Move your knee and ankle as much as possible to avoid getting stiff. After 6 weeks you will be allowed to begin weight bearing.
Blood Clot Prophylaxis
Patients with pelvis and leg fractures are at risk to get blood clots in the legs that can dislodge and travel in the bloodstream to the lungs causing disability or death. There are several ways to decrease the risk of this complication. In the hospital you are given shots in the belly called Lovenox and have pneumatic compression devices on your legs. Once discharged home take one baby aspirin(81mg) a day for 2 weeks. Walking and moving as much as you can is also preventative.
Physical Therapy
Most patients with distal femur fractures require physical therapy. This usually starts at your first postoperative visit. Usually, patients do 1-2 visits with the therapists a week and must continue these exercises at home daily for a good result. For the first 6 weeks this consists of range of motion and modalities while the bone begins to heal. At 6 weeks it progresses to stationary bike riding and more aggressive range of motion. Most patients need about 3-4 months of therapy to regain their preinjury range of motion and strength.
Return to Work
Patients can usually return to a desk job or light duty after a few days. Return without restriction to jobs that require heavy lifting or manual labor usually takes about 12 weeks.
Driving
You should not drive with your operative leg until 6 weeks after surgery.
Hardware Removal
The plate and screws usually stay in for life and are not routinely removed. However, if the metal becomes infected or is painful 1 year after surgery it can be removed. If patients develop posttraumatic arthritis and require a knee replacement the hardware will need to be removed.
Healing Time
Distal femur fractures treated with surgery take about 3-4 months to heal completely. Younger patients heal slightly faster and older patients or those with diabetes take slightly longer to heal.