Artificial Lumbar Disc Surgery
What is a Disc?
The spine is a column that is made of up bones, discs and ligaments. The blocks of bone (or vertebrae) provide the anterior support and structure of the spine. The discs are in between the bones and act like a “shock absorber” between the vertebrae. The discs also contribute to the flexibility and mobility of the spinal column. The discs are made up of two parts:
- The inner portion of the disc is a jelly-like material and is called the nucleus pulposus and
- The outer part, called the annulus fibrosis of the disc, is stronger and more fibrous. The annulus fibrosis surrounds and supports the inner jelly material. The annulus is rich in nerve fibers, especially the back portion, and may play a role in the production of discogenic back pain.
Disc material is mainly composed of water and other proteins. As a normal part of aging, the water content gradually reduces. This can cause the disc to flatten out and even develop tears or cracks throughout the annulus fibrosis. These discs are often referred to as “degenerative” discs and may or may not cause pain.
In the case of a degenerative disc, the inner jelly material (the nucleus pulposus) can bulge out and press up against the annulus fibrosis. This can stimulate the pain receptors causing pain to occur. The cracks or tears that develop within the annulus fibrosis can also become a source of pain. Finally, the inner nucleus can also come out through the cracks in the annulus and compress nerves or spinal cord, a condition that may cause weakness, pain, pins and needles or numbness, and may require surgery.
Current Treatment Options for Lumbar Disc Disease
Non-surgical options for people with disc protrusions in the lower back include rest, heat, pain medications and physiotherapy. When non-surgical treatment options fail, surgery is often the next step. This usually means spinal fusion surgery. Back pain with compression of the nerves in the neck or spinal cord is a common condition that affects the spine and may require surgery. If only nerves are compressed, with symptoms in one or both legs, a period of conservative management is instituted and if this fails surgery is contemplated. Typical surgical procedures for ongoing leg symptoms include lumbar microdiscectomy of lumbar laminectomy. These operations do not address back pain. Occasionally, a spinal fusion is performed for back pain or for back pain in association with leg symptoms. All these procedures are performed from a posterior approach which involves a degree of muscle stripping in order to expose the bony structures.
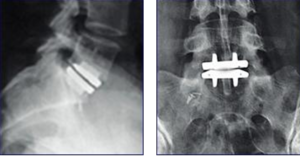
Spinal fusion is typically performed from a posterior approach in the lumbar spine, using screws, rods, cages and bone graft from the hips. there is an extensive recovery period and the back becomes stiffer. If a fusion is required or if a large component of the pain is back pain, then a posterior approach is necessary. Occasionally, for pure back pain, thought to be coming from the discs, an anterior fusion is performed, with or without a posterior fusion.

(Above): Typical lumbar fusion with screws, cages, rods and bone graft performed for lumbar disc disease:
The main problems with fusing bones in the lower back are that adjacent levels in the lumbar spine are placed under more strain. This is particular common with posterior lumbar fusions and less so anterior ones. This has increased “wear and tear” at the surrounding disc space levels has been termed “adjacent segment disease”. We now know that if 10 people have a single level fusion, at 10 years two have had to have another operation for narrowing at the next level either above or below. Secondly, the bone does not always heal or “fuse” correctly. In fact, the overall success rates for these procedures range from 40% to 90%. Movement is also lost, with a loss of movement at one or more levels.

(Above): Wear and tear above a previous fusion (arrows)
Lumbar Disc Replacement Instead of Lumbar Fusion
A new technique which has been available in Europe for the past 11 years is removing the disc and then replacing it with an artificial disc. This has two main benefits:
- Motion is maintained and the patient will not feel a restriction in the range of motion.
- Theoretically adjacent segment disease will not occur.
Consequently, patients undergoing placement of an artificial lumbar disc may need less surgeries on their back in the future.
The idea of spinal disc replacement is not new. It was first attempted 40 years ago when implanted stainless steel balls were implanted into the disc spaces of over 100 patients. These pioneering efforts were followed by more than a decade of research on the degenerative processes of the spine, spinal biomechanics and biomaterials before serious efforts to produce an artificial disc resumed. There are currently a number of artificial disc prosthesis available on the market:
Prodisc® Disc Prosthesis

Charite® Disc Prosthesis
Maverick® Disc Prosthesis
Others
Both the Prodisc and the Charite have the longest track record in terms being used in patients, with the Prodisc having been used clinically for 11 years, far longer than the scenario in the cervical spine.
Indications
Not all patients with back pain are suited to placement of an artificial lumbar disc prosthesis. The ideal candidate has the following features:
- Back pain thought to be coming from the discs, not the facet joints.
- No previous surgeries other than a lumbar microdiscectomy
- Not markedly overweight
- Relatively few if any abdominal operations
- Little in the way of leg symptoms

Part of the workup for potential artificial disc placement includes plain x-rays, MR scanning, facet blocks and a lumbar discogram. The latter study involves injecting the suspect lumbar discs with saline to see if the exact same pain is reproduced that is concerning the patient. Adjacent discs are also injected and used as controls. The procedure is painful but absolutely necessary and is performed by a skilled neuroradiologist in a CT scanner. Occasionally an abdominal angiogram is also required.
Technique of Artificial Lumbar Disc Placement
The surgery takes 2-3 hours and is performed through a 10 cm incision in the abdomen. The main risks of the procedure are that the large veins and arteries from/to the legs need to be dissected away from the front of the disk. There is a risk of injuring these vessels with major bleeding requiring transfusion or possibly even death. The risk of a disaster happening is 1-3%. Occasionally more than one level is operated upon in which case the risks get higher. Men have a risk of developing retrograde ejaculation after surgery, which may render them infertile. It is a good idea for men planning on families in the future to donate sperm preoperatively. The other risks including infection, abdominal problems etc etc gives a 5% overall risk of something bad happening. Typically, if the disc is abnormal on MR with a positive provocative discogram, the success in terms of pain relief is about 70%.
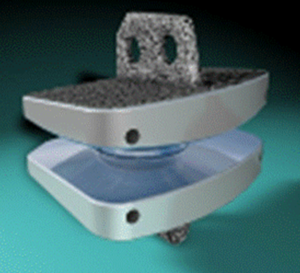
The Prodisc® consists of two outer metal parts with an inner polyethylene core that makes it a ball and socket joint (see below). Other devices come in one or three pieces:

Initially the disc space to be operated upon is identified and removed:

Note that the nerves themselves are not decompressed.
The individual components of the Prodisc® are then inserted in sequence to replace the original disc. Some devices are assembled in situ (Charite):

The final result is removal of the disc, with (hopefully) removal of the pain generators at the back of the disc, and placement of a prosthesis that will allow movement in all normal planes:
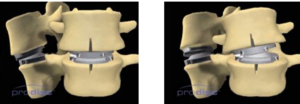
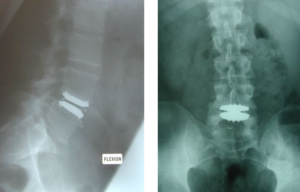
FLEXION/EXTENSION LATERAL BENDING
Results of Artificial Lumbar Disc Placement
In the best cases, 70-90% of patients will get relief of the back pain
The operation is not for leg pain
The risk of complications is about 5%. There is a very small of chance of something happening like dying. There is a higher chance, however of needing revision surgery than an anterior fusion and at the moment we do not know what long term benefits this operation conveys over an anterior fusion.
Risks and Complications
Death or major nerve/blood vessel injury/massive transfusion 1-2%
All other complications including bleeding, infection, abdominal complications, blood clots etc. 5%
Retrograde ejaculation (impotence) in men 5-10%
Recovery
Hospitalization is typically for 2-5 days
A brace must be worn for three months
Extension of the back must be avoided
Swimming can be commenced after four weeks
No sporting activities, golf or tennis to be undertaken for three months
Running after six weeks
X-rays will be done immediately after surgery, at six weeks, three months, six months then yearly to ensure the prosthesis is not moving (see below). A survey form is also completed
Non-Surgical Options
Despite the length discussion about surgery, most patients get better without surgery.
Conservative therapy comprises
- Analgesia with NSAIDs (e.g. Mobic, Voltaren or Celebrex)
- Analgesia with other medications such as Tramadol
- Avoidance of bending/lifting/twisting/sitting for prolonged periods
- Physiotherapy
- Hydrotherapy
- Perineural/intrafacet steroid and local anesthetic injections
- Possibly acupuncture
- Seeing a Pain Management Centre about spinal stimulators, pumps and pain management programs
Your surgeon and primary care doctor can tailor a conservative management plan with some or all of the following, and for the vast number of sufferers, conservative management works. There are other alternative therapies available, but many have shaky scientific foundations and consequently are best avoided. Spinal manipulation is best avoided as it can entice more disc material to prolapse.
IMPORTANT POINTS
- The selection of patients for this surgery is very particular and left to very specialized neurosurgical and orthopedic spinal surgeons
- We do not yet know the long term outcomes of having an artificial disc for 50+ years
- Over 2000 Prodiscs® have been placed in patients in Europe over the past 12 years and none have been removed. Over 10000 Charite® devices have been placed over the past 20 years. Other devices have only been used for 2-5 years.
- The aim is to keep movement at the level of surgery so that extra stress is not placed at the adjacent level.
- The operation is good for back pain (70% likely to improve) but will not change leg symptoms.
- The risk of something disastrous happening from the surgery such as death, massive bleeding or sever nerve injury is 1-2%. The risk of other complications is about 5-10% which included the risks of infection, bleeding etc. etc. There is a 10% in males of developing retrograde ejaculation which would render the patient infertile. Sperm donation prior to the surgery for patients contemplating surgery is a good idea if they are still planning on having a family. a
- The long term results with artificial discs are not yet known. In the lab, the discs have been tested to an equivalent of 15 years with little wear. We do know that hip and knee replacements do wear out and the same may happen with this prosthesis- at this stage we just don’t know. I suspect not many people will need them revised but it may take 10-20 years to find out. Significantly, very few have been removed to date. I personally would have a prosthesis over a fusion, if indicated, despite the long term uncertainty.
- At this stage it is only very few fusion patients who qualify for this procedure.