Disc Herniations, Sciatica and Microdiscectomy
Definition
Lumbar discectomy encompasses a number of terms, including discectomy, microdiscectomy and laminectomy/discectomy. The typical patient presents with pain down one leg which may radiate from the buttock to below the knee. The usual pain is either to the back of the calf and to the sole of the foot, or to the outside of the shin and top of the foot. Back pain is not usually a feature, however it may initially occur. Lumbar disc problems are exceedingly common and it is important to realize that in the vast majority of cases non-operative management works very well. Most patients settle within 6-12 weeks after the onset of symptoms. The pathophysiology of why a patient gets symptoms is disc protrusion is complex. The anatomy of a typical intervertebral disc as shown below:
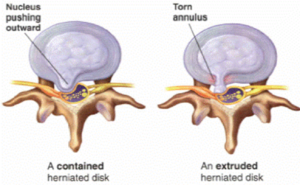
(Below): The intervertebral disc lies in front of the spinal nerves and is situated between the vertebral bodies. It carries 80% of the load through that level and is the shock absorber for the spine. The lowermost discs (L45 and L5S1) are most prone to wear and tear and potential rupture.
Note that there is an outer shell, called the annulus fibrosis and an inner core called the nucleus pulposus. The annulus is the consistency of a pencil eraser, whereas the nucleus is gel-like and, as we get older, dehydrates and becomes like crabmeat. The discs act as shock absorbers and flexing the spine loads the disc. A tear in the outer annulus can consequently cause severe back pain. Patients will often be able to remember a time when they lifted poorly or twisted their back and had severe back pain prior to getting the leg pain. Once an annular tear occurs, it may heal, or it may allow nucleus to come out of the centre of the disc, into the spinal canal, where it may compress nerves. This is usually called one of a number of terms, including “disc prolapse”, “ruptured disc”, “slipped disc”, “extruded disc” etc. All these terms essentially mean the same thing. Once nerves are compressed, surgery may be complicated. It is important to know that the prolapsed disc cannot be pushed back into place and nothing but time will heal the annular tear. Thus, in general, any surgery is aimed at improving the leg pain, not the back pain.
Anatomy
If you study the MRI and CT scan shown below, the reason for symptoms from a disc protrusion become evident.
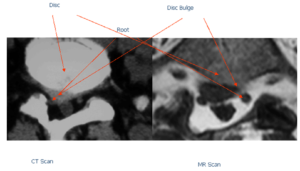
A disc protrusion per se may not cause symptoms. If the annulus is acutely torn, back pain may result, but the management is usually not operative. If the disc pushes on a nerve, as shown in the previous CT and MRI scan, then symptoms down one or occasionally both legs may result. The symptoms can include pain, numbness, “pins and needles”, and weakness.
Reason For Operation
Lumbar disc protrusions are not usually operated upon early, but there are some clear situations when a surgeon may recommend early surgery. If there is evidence of severe weakness, early surgery may be offered. If the pain in the leg is so severe that narcotic analgesia is not controlling the pain, early surgery may again be an option. Finally, if there is a suggestion of problems with the nerves that supply the bladder or bowel, early surgery is advocated. In this latter situation, an inability to pass urine may be evident, or there may be numbness in the crotch area, buttocks or when passing urine. This situation usually necessitates emergent or early surgery.
If a patient has pain, but it is not too severe, then typically conservative management is initiated. It must be remembered that the vast proportion of patients will settle with time and as long as improvements are noted at 6 weeks, there is minimal or no weakness, and the pain is not excruciating and is livable with oral analgesia, then waiting and continuing with conservative therapy is a good option.
If weakness occurs and is not improving, surgery is usually offered. Similarly, if symptoms are not improving at 6 weeks then surgery is an option.
In most cases, when managing just leg pain, surgery is a treatment option that speeds up the rate of recovery, remembering that most cases will get better by themselves. Again, specific recommendations are tailored to the patient. In the vast number of cases, the goal is control of pain, and an intervention that achieves this and is less invasive than surgery is a reasonable option.
Technique
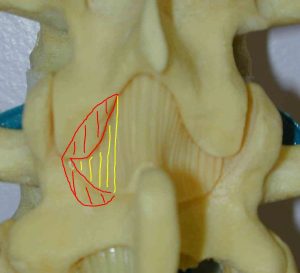
If surgery is undertaken, it is usually performed as a minimally invasive procedure. The procedure can be performed as a day stay surgery. General anesthesia is utilized and the surgery is performed through an incision of 3-5 cm. Much emphasis is placed on performing the surgery through tiny incisions (so called “microendoscopic” discectomy) although, for the most part, the surgery can be performed more safely and quickly via a standard approach, with little tangible gain through a slightly smaller incision. Usually a small window is made on one side of a spinous process through the removal of some bone (shaded red) and ligament (shaded yellow) to allow visualization of the disc bulge and involved root. This is shown below :
Through gentle dissection under illumination and magnification, the interface between the root and disc bulge is identified and the offending fragment is removed. Only a small portion of disc is removed. The whole disc is not removed, although any loose fragments felt through the hole in the annulus are removed. The tear in the annulus is not repaired. After the nerve is freed completely the operation is completed. Typically this takes 0.5- 1.5 hours to perform.
Risks
The greatest risk is injury to one or more nerves and this is typically les than 1%. The risks of infection, bleeding etc. etc. are similar to those for a laminectomy as are the risks of general complications. 10-15% of patients will have a recurrent disc protrusion, either at the same side and level or at different levels or the opposite side. The greatest risk for this is in the first 6 weeks after surgery.
The small but real risks from surgery are the reason why all patients with disc protrusions do not immediately have surgery.
Expectations
In uncomplicated cases the likelihood of good/excellent relief of leg pain is 80-90%. Numbness is slow to recovery and may persist. Weakness also may take 6-12 weeks to return to normal. Pins and needles usually starts to improve immediately.
Recovery
Patients who have a lumbar discectomy are typically in hospital for the day or one night. They are advised not to work for 2 weeks and recommendations on back and wound care are the same as for lumbar laminectomy. It is notable that bending, lifting and twisting may increase the recurrence rate in the first 6 weeks, so my patients do not do any other exercise other than walking for that time period. After 6 weeks a return to normal activities is initiated. It is important to remember that the back is not normal after disc surgery and that care needs to be taken in the future. Bending, lifting and twisting need to be avoided as these activities ultimately may have precipitated the initial event. Recovery from surgery is not a license to return to normal. Good back care is the rule for life.
Again, as is the case after lumbar laminectomy, no surgeon can guarantee risk-free surgery or a 100% good outcome.
Non-Surgical Options
Despite the length discussion about surgery, most patients get better without surgery.
Conservative therapy comprises
- Analgesia with NSAIDs (e.g. Mobic, Voltaren or Celebrex)
- Analgesia with other medications such as Tramadol
- Avoidance of bending/lifting/twisting/sitting for prolonged periods
- Physiotherapy (traction may help)
- Hydrotherapy (particularly if back pain is a problem)
- Perineural steroid and local anesthetic injections
- Possibly acupuncture
Your surgeon and primary care doctor can tailor a conservative management plan with some or all of the following, and for the vast number of sufferers, conservative management works. There are other alternative therapies available, but many have shaky scientific foundations and consequently are best avoided. Spinal manipulation is best avoided as it can entice more disc material to prolapse.
In the first four weeks after disc prolapse, a large amount of inflammation occurs around the nerve root and this can contribute to pain. NSAIDs at this time can reduce pain and are most effective for acute sciatica. Interestingly, over time the disc bulge tends to dehydrate and shrink. It never retracts back into the disc space but on subsequent imaging can be reduced in size. This shrinking phenomenon is most prevalent with large protrusions. The size of a disc bulge also has no correlation to symptoms; unless a cauda equina syndrome is present a large bulge does not-by virtue of its size-absolutely have to be removed.
Other Points
To emphasize, lumbar discectomy is a good operation for leg and buttock pain, not back pain and most of these disorders get better without surgery. In general if symptoms still persist in a fashion that interferes with a patient’s quality of life after 6-12 weeks, surgery is a definite treatment option.
Copyright © 2010 All rights reserved.